ANTIBODIES PRODUCED
Cross-reactive
autoimmune antibodies
are produced to destroy
the infectious organism.

TARGET BASAL GANGLIA
Cross-reactive autoimmune
antibodies mistakenly target
healthy cells in the basal
ganglia region of the brain.

NEURONAL TARGETS
These autoimmune antibodies
can bind to or block neuronal
targets in the brain.
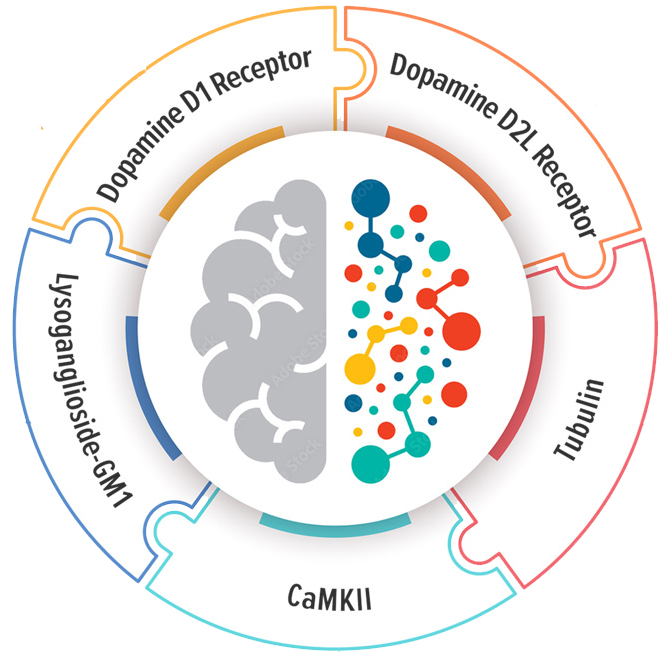
(Dopamine D1 and D2 receptors,
Lysoganglioside GM-1, Tubulin

{kind=link}
{kind=link}
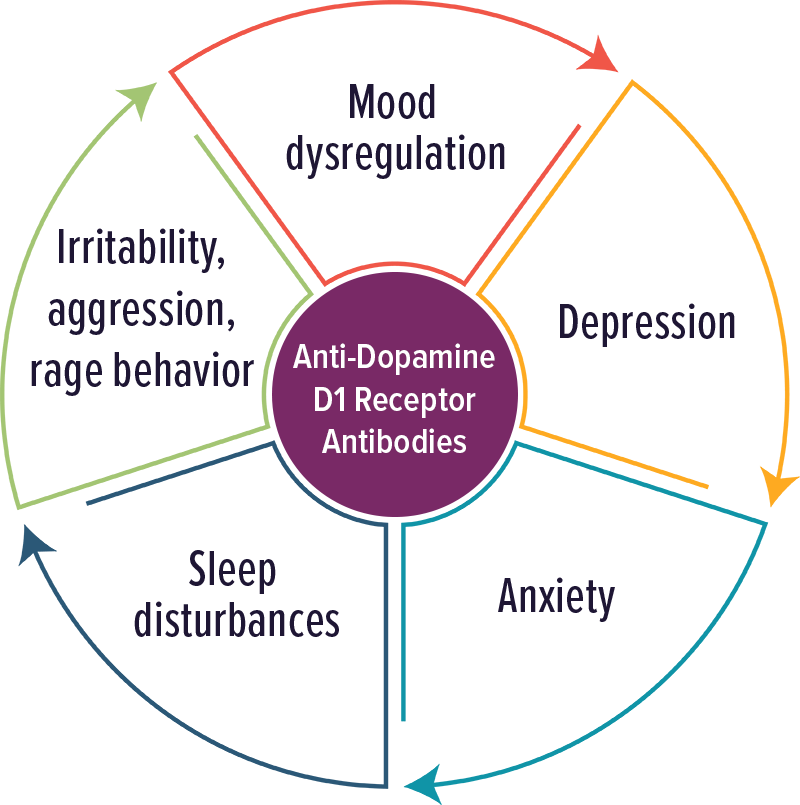
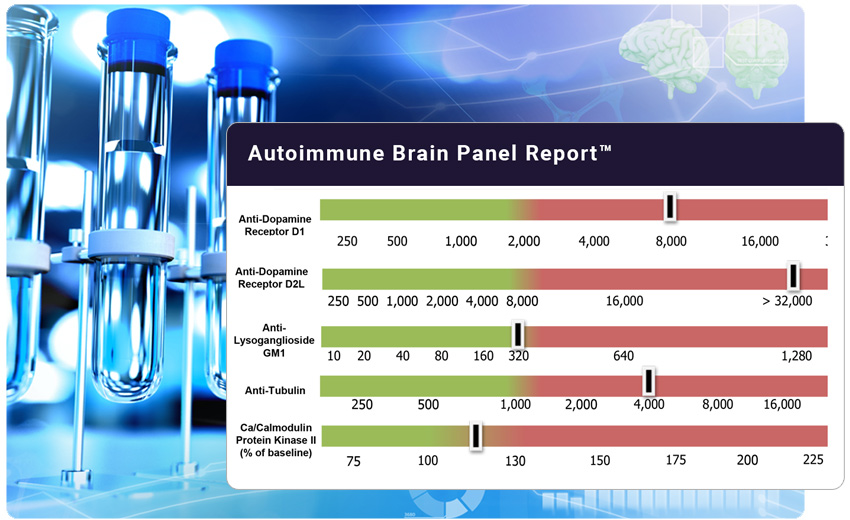
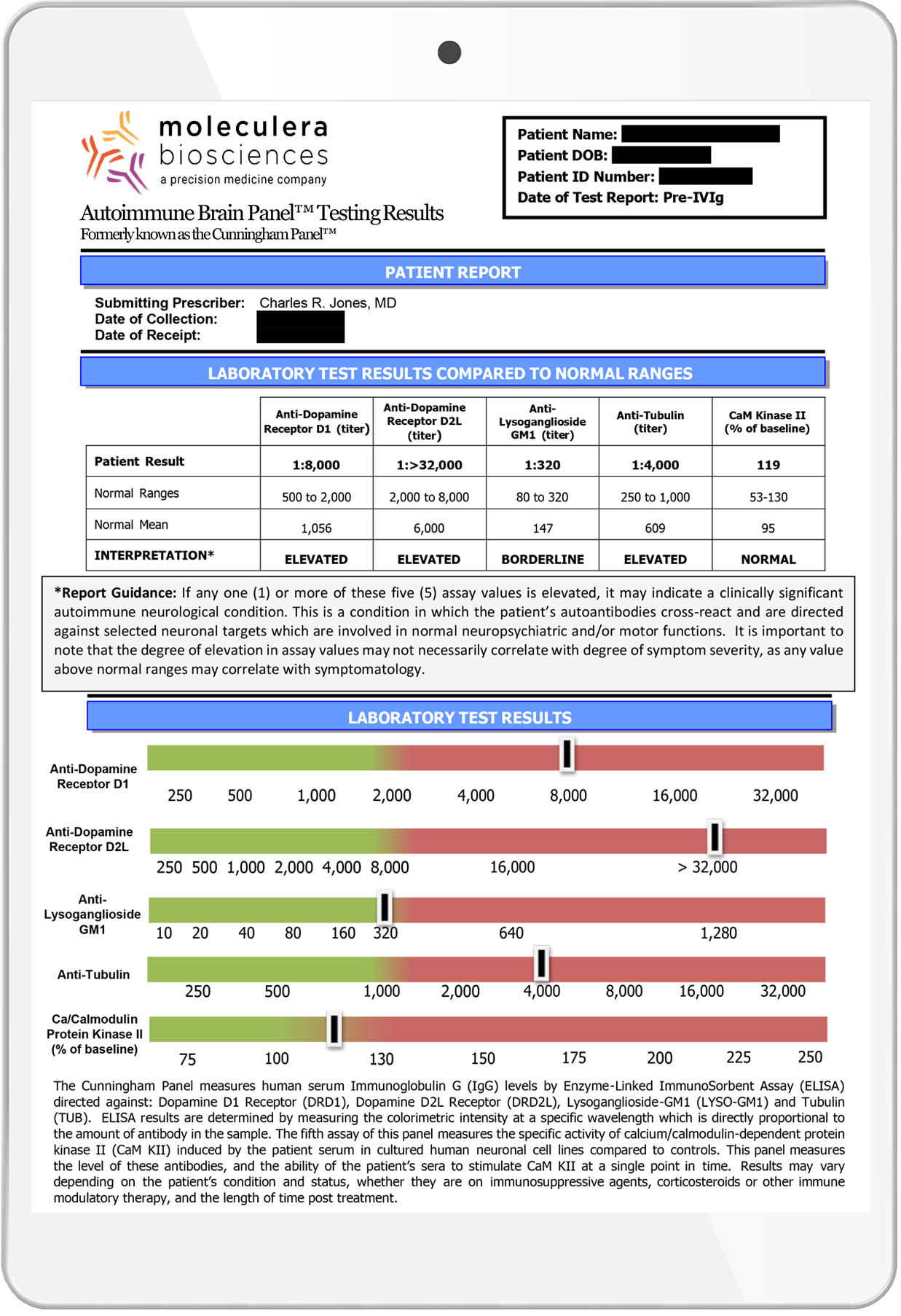
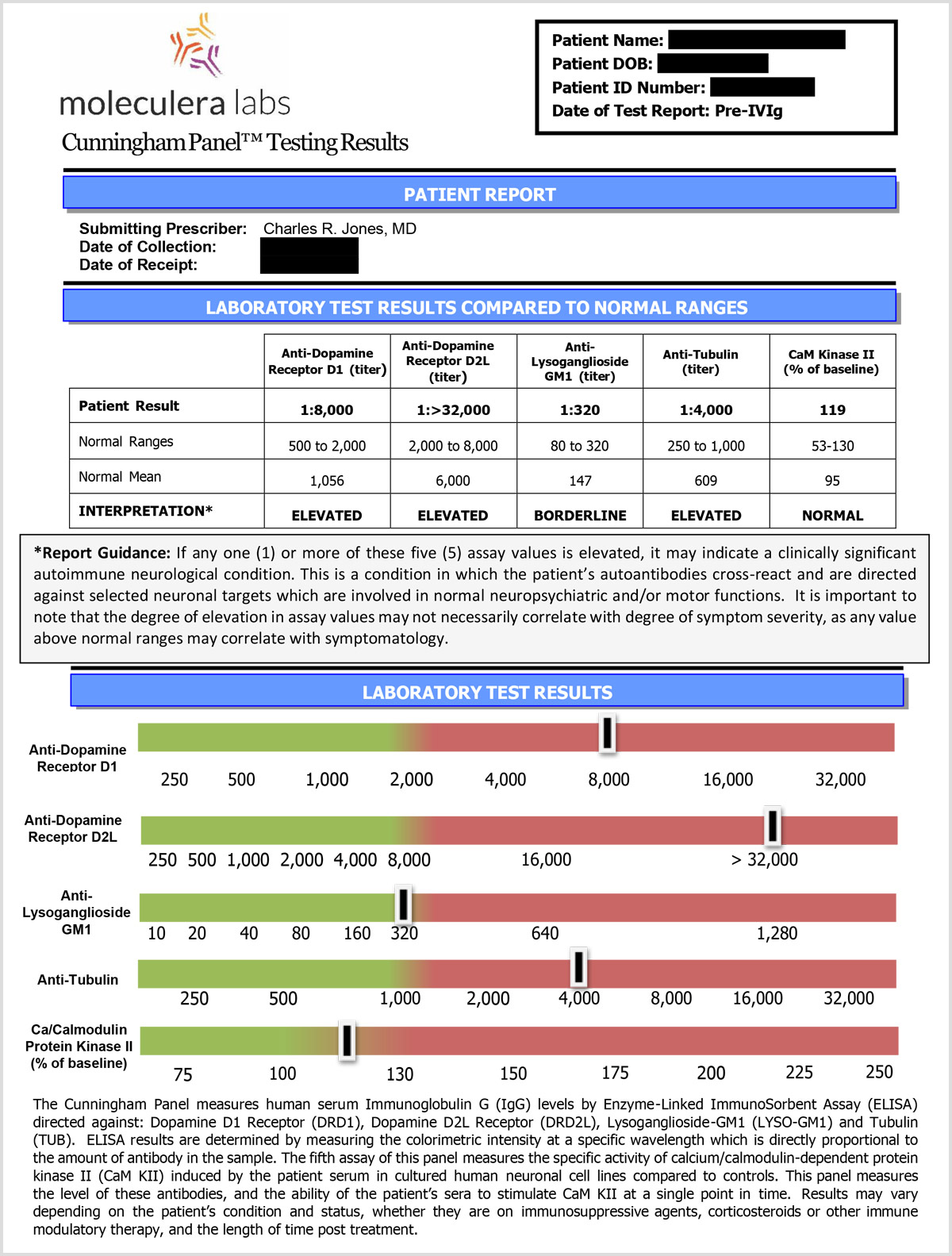
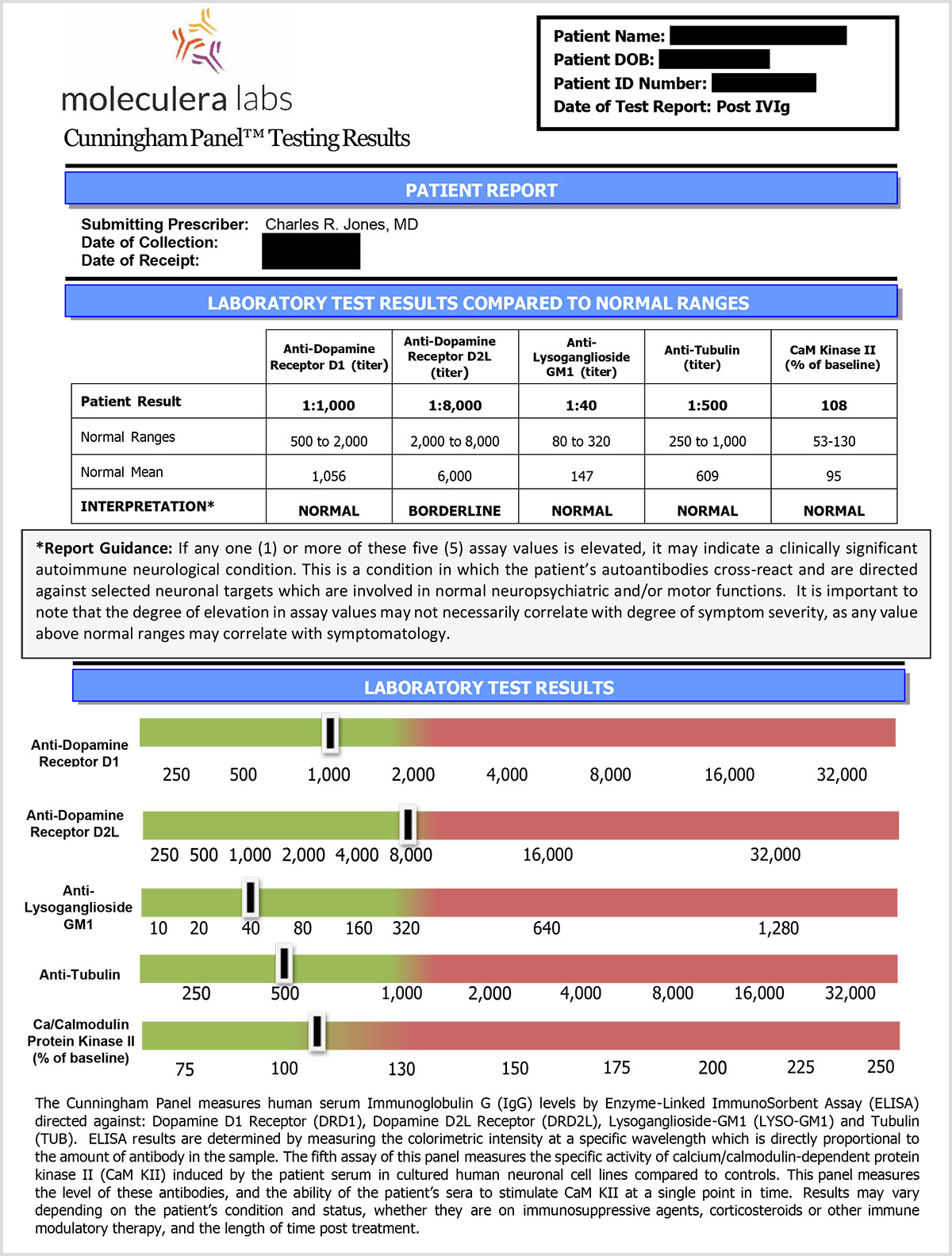
Dopamine D1 Receptor Antibodies
Individuals with elevated levels of autoantibodies against Dopamine D1 receptor typically experienced psychiatric symptoms, including psychosis. Other symptoms included: mood dysregulation, anxiety, depression, sleep disturbances, irritability, aggression and rage behavior.
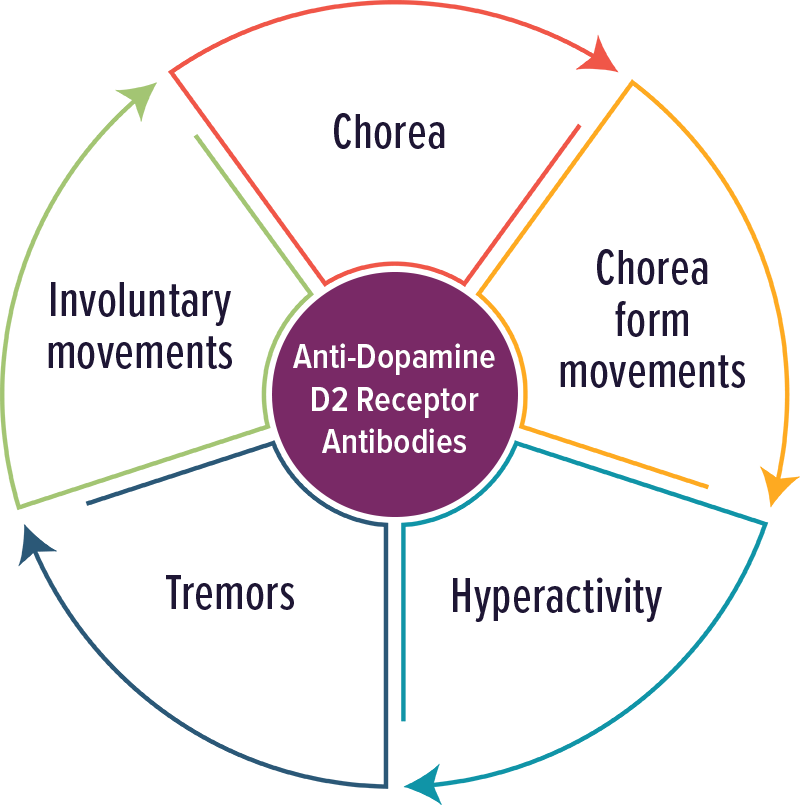
Dopamine D2 Receptor Antibodies
Individuals with elevated levels of autoantibodies against Dopamine D2 receptor typically experienced movement disorders and impulsivity. Other symptoms included: chorea, chorea form movements, hyperactivity, tremors and involuntary movements.
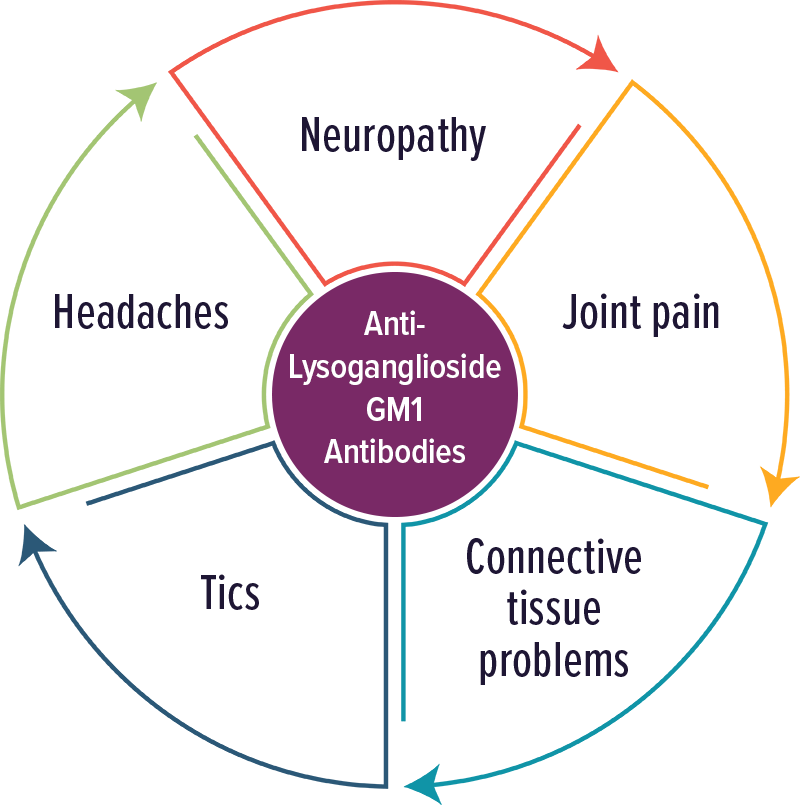
Lysoganglioside GM1 Antibodies
Individuals with elevated levels of autoantibodies against Lysoganglioside GM1 typically experienced neuropathic symptoms, including tics. Other symptoms included: neuropathy, joint pain, connective tissue problems, tics and headaches.
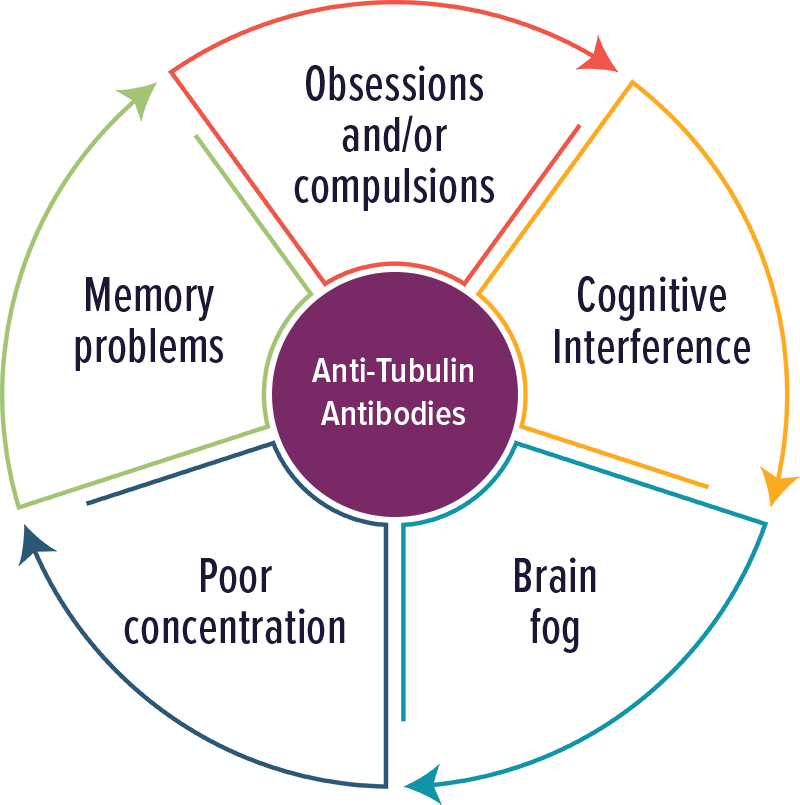
Tubulin Antibodies
Individuals with elevated levels of autoantibodies against Tubulin typically experienced cognitive complaints, OCD and brain fog. Other symptoms included: poor concentration and memory problems.
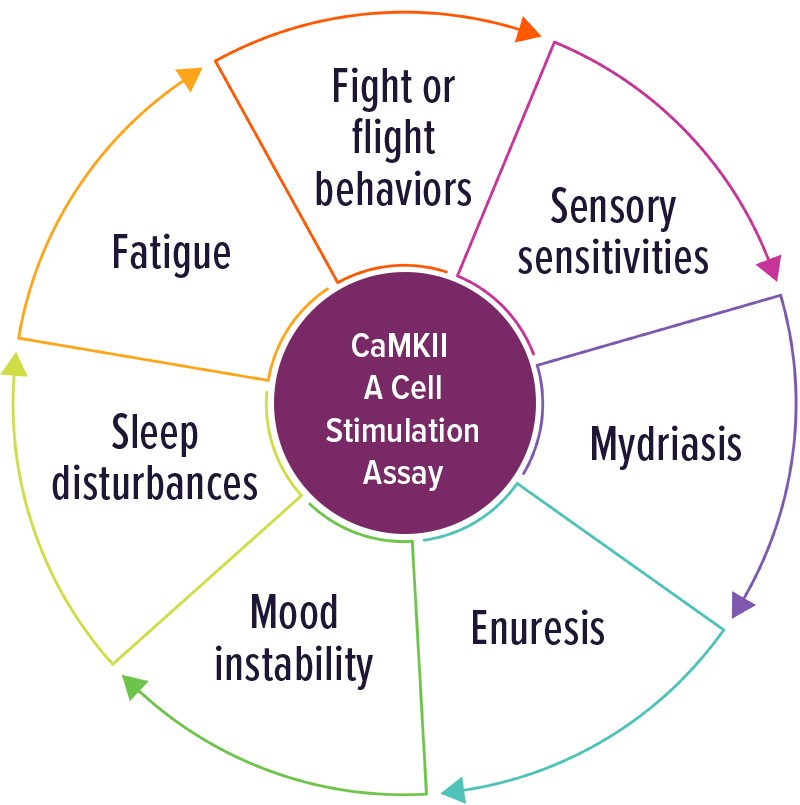
CaMKII – A Cell Stimulation Assay
Individuals with elevated CaMKII levels were often positive with involuntary movements and any symptom of adrenergic activation. Other symptoms included: fight or flight behaviors, sensory abnormalities, fatigue, sleep disturbance, mood instability, enuresis and mydriasis.