Basal Ganglia Encephalitis
Recognizing autoimmune-induced neuropsychiatric symptoms
Encephalitis of the brain can trigger changes in behavior
Encephalitis, which refers to inflammation of the brain, can occur in various regions of the brain. Encephalitis of the brain is typically caused by an infection (infectious encephalitis) or autoimmune reaction (autoimmune encephalitis).
Autoimmune encephalitis (AE) occurs when the body’s immune system produces antibodies that mistakenly attack portions of the brain. These autoantibodies target receptors or proteins in different regions of the brain, which can result in a range of neuropsychiatric symptoms. 1
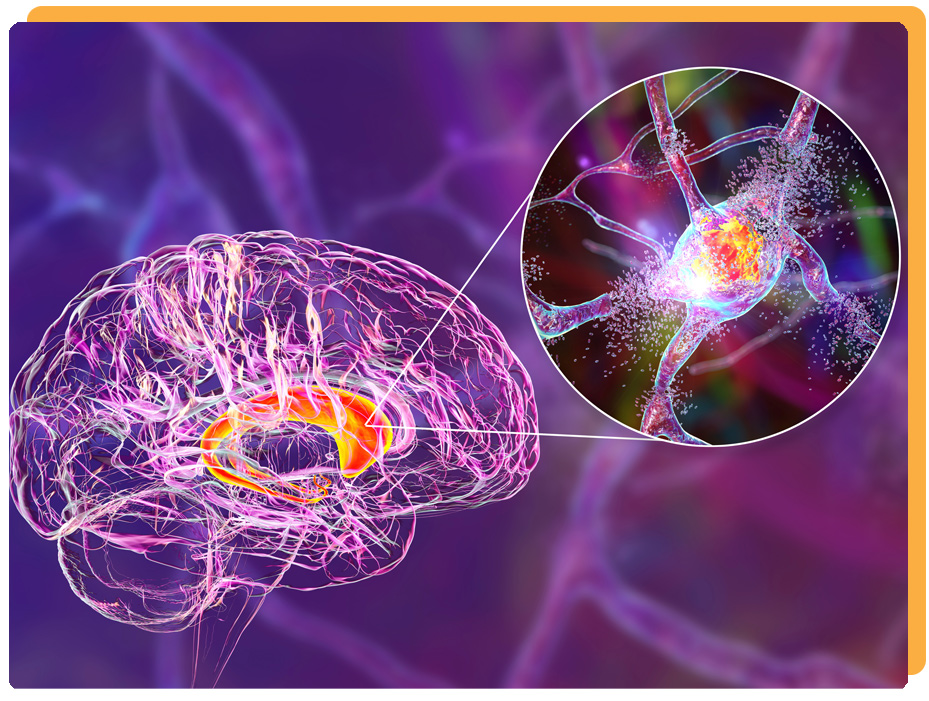
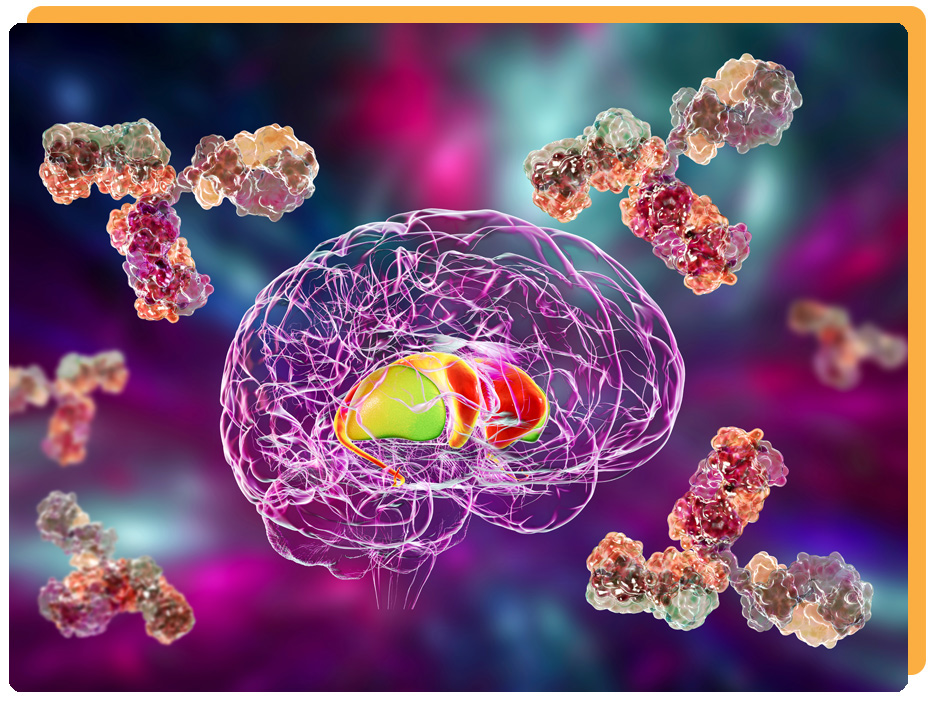
Basal ganglia encephalitis occurs when autoantibodies attack the brain
In recent years, the number of confirmed cases of AE [autoimmune encephalitis] has been increasing annually, as a growing number of neuronal autoantibodies are discovered. 2
There are different forms of autoimmune encephalitis, each defined by the antibodies involved and the targets within the brain. Basal ganglia encephalitis (BGE) can occur when autoantibodies attack an area of the brain known as the basal ganglia. PANS and PANDAS are a types of basal ganglia encephalitis. 3
Basal ganglia encephalitis, which may be caused by an underlying infection, can trigger neurologic and psychiatric symptoms, such as obsessions/compulsions, anxiety, depression, mood swings and other changes in behavior. 3
Testing with the Autoimmune Brain Panel™ can assist clinicians in diagnosing and treating basal ganglia encephalitis. One study found that the antineuronal antibodies measured with the Panel can serve as biomarkers for BGE. 3
Autoimmune Brain Panel helps identify autoimmune-induced neuropsychiatric symptoms
Dr. Craig Shimasaki discusses how the Autoimmune Brain Panel (also known as the Cunningham Panel) can assist clinicians in determining whether neuropsychiatric symptoms, such as OCD, tics, anxiety, mood changes, may be caused by an infection-triggered autoimmune dysfunction.
It is important to know whether psychiatric symptoms, neurologic manifestations or changes in behavior or personality are due to an autoimmune encephalopathy, such as basal ganglia encephalitis, rather than a primary psychiatric illness. With the proper treatment, symptoms can be greatly reduced or completely resolved.
For example, some of the approaches to treatment may involve identifying and eradicating possible underlying infections, treating a dysfunctional immune system and reducing inflammation or encephalitis of the brain. Published treatment guidelines have listed immunomodulatory therapies, anti-infective medications, antibiotics, anti-inflammatory drugs, steroids, IVIG or plasmapheresis. 4
Why is it important to identify and treat?
“Over the past 10 years, identification of autoimmune forms of encephalitis with antibodies against neuronal surface antigens … have shown that CNS disorders … can be antibody mediated and benefit from immunomodulatory therapies.” 7
Treatment for basal ganglia encephalitis is different and often involves anti-infective and immunomodulatory therapies. 4
Early diagnosis and treatment has been shown to improve chances for a full recovery. 8
With proper treatment, symptoms/behaviors are often resolved with significant improvement in symptoms or a complete remission. 9
References
- Platt MP, Agalliu D, Cutforth T. Hello from the Other Side: How Autoantibodies Circumvent the Blood-Brain Barrier in Autoimmune Encephalitis. Front Immunol. 2017;8:442. Published 2017 Apr 21. doi:10.3389/fimmu.2017.00442
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5399040/ - Gu Y, Zhong M, He L, et al. Epidemiology of Antibody-Positive Autoimmune Encephalitis in Southwest China: A Multicenter Study. Front Immunol. 2019;10:2611. Published 2019 Nov 12. doi:10.3389/fimmu.2019.02611
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6861323/ - Chain JL, Alvarez K, Mascaro-Blanco A, et al. Autoantibody Biomarkers for Basal Ganglia Encephalitis in Sydenham Chorea and Pediatric Autoimmune Neuropsychiatric Disorder Associated With Streptococcal Infections. Front Psychiatry. 2020;11:564. Published 2020 Jun 24. doi:10.3389/fpsyt.2020.00564
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7328706/ - Jennifer Frankovich, Susan Swedo, Tanya Murphy, Russell C. Dale, Dritan Agalliu, Kyle Williams, Michael Daines, Mady Hornig, Harry Chugani, Terence Sanger, Eyal Muscal, Mark Pasternack, Michael Cooperstock, Hayley Gans, Yujuan Zhang, Madeleine Cunningham, Gail Bernstein, Reuven Bromberg, Theresa Willett, Kayla Brown, Bahare Farhadian, Kiki Chang, Daniel Geller, Joseph Hernandez, Janell Sherr, Richard Shaw, Elizabeth Latimer, James Leckman, Margo Thienemann, and PANS/PANDAS Consortium.Journal of Child and Adolescent Psychopharmacology.Sep 2017.574-593.http://doi.org/10.1089/cap.2016.0148
https://www.liebertpub.com/doi/full/10.1089/cap.2016.0148 - Zuliani L, Graus F, Giometto B, Bien C, Vincent A. Central nervous system neuronal surface antibody associated syndromes: review and guidelines for recognition. J Neurol Neurosurg Psychiatry. 2012 Jun;83(6):638-45. doi: 10.1136/jnnp-2011-301237. Epub 2012 Mar 24. PMID: 22448032; PMCID: PMC3348613.
https://pubmed.ncbi.nlm.nih.gov/22448032/ - Chang K, Frankovich J, Cooperstock M, et al. Clinical evaluation of youth with pediatric acute-onset neuropsychiatric syndrome (PANS): recommendations from the 2013 PANS Consensus Conference. J Child Adolesc Psychopharmacol. 2015;25(1):3-13. doi:10.1089/cap.2014.0084
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4340805/ - Graus F, Titulaer MJ, Balu R, et al. A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol. 2016;15(4):391-404. doi:10.1016/S1474-4422(15)00401-9
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5066574/ - Shin Y-W, Lee S-T, Park K-I, et al. Treatment strategies for autoimmune encephalitis. Therapeutic Advances in Neurological Disorders. January 2018. doi:10.1177/1756285617722347
https://journals.sagepub.com/doi/pdf/10.1177/1756285617722347 - Brenton JN, Goodkin HP. Antibody-Mediated Autoimmune Encephalitis in Childhood. Pediatr Neurol. 2016 Jul;60:13-23. doi: 10.1016/j.pediatrneurol.2016.04.004. Epub 2016 Apr 12. PMID: 27343023.
https://www.pedneur.com/article/S0887-8994(15)30139-9/pdf